LET US HELP

Welcome to Capella
Select your program and we'll help guide you through important information as you prepare for the application process.
LET US HELP
Welcome to Capella
Select your program and we'll help guide you through important information as you prepare for the application process.

Which degree is right for you? MBA vs MS in Human Resource Management
April 10, 2024
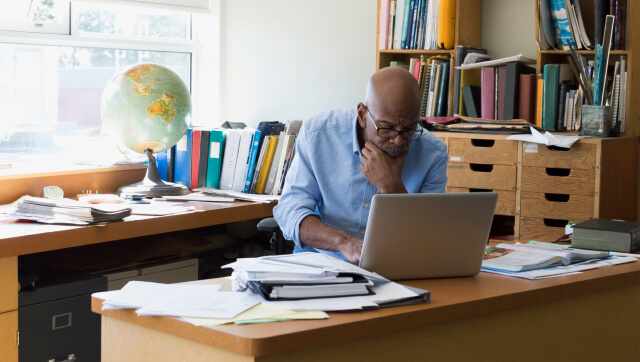
How organizations can walk the talk when it comes to work-life balance
November 05, 2019
Ten questions with Capella human resources faculty chair Shelley Robbins, PhD
October 31, 2014
Triple aim: strategies to create a new health care model that works
December 19, 2018
Tell it like it is – honesty in communicating organizational culture
December 27, 2019
Job interview basics: how to answer common interview questions with confidence
November 12, 2019
How organizations can walk the talk when it comes to work-life balance
November 05, 2019
Ten questions with Capella human resources faculty chair Shelley Robbins, PhD
October 31, 2014
The relationship between competency-based education and direct assessment
November 08, 2017
Marriage and family therapy & social work degrees: How to tell the difference
October 03, 2023
How counseling is changing to meet the needs of today’s older adults
November 18, 2019
Help youth succeed in school and life with a behavioral health degree
August 02, 2019
Collaborative efforts in counseling, clinical psychology, and social work
June 28, 2019
Transforming lives: making a career as a marriage and family therapist
March 29, 2019
Collaborative efforts in counseling, clinical psychology, and social work
August 21, 2018
10 questions with Capella counseling faculty member Benjamin Noah, PhD
April 14, 2015
Ten questions with Capella counseling faculty member Leslie Korn, PhD
December 11, 2014
Professional development for teachers: taking EdTech to the next level
August 23, 2017
Ten questions with Capella education faculty member Dana Sparkman, PhD
October 14, 2015
In the field: how K-12 teachers are using technology in the classroom
September 21, 2015
Administration or management: guide to bachelor’s degrees in health care
May 07, 2019
Triple aim: strategies to create a new health care model that works
December 19, 2018
What you need to know about the Merit-based Incentive Payment System (MIPS)
November 15, 2018
Generational differences in public health and health administration
February 21, 2017
Three strategies for career success in an artificial intelligence-driven world
December 12, 2018
Announcing Capella University’s 2018 women in analytics scholarship winners
September 17, 2018
4 areas of interest at the intersection of technology and health care
February 07, 2018
Capella and SAS announce 2017 scholarships for women in analytics
September 18, 2017
Capella VP takes unlikely path to career in data analytics and business strategy
May 01, 2017
Four benefits of speaking with a Capella student before you enroll
October 21, 2018
Capella faculty member and astronomer suggests answer to 4 billion-year-old paradox
March 09, 2017
Capella University earns approved education provider status from NAADAC, the association for addiction professionals
March 15, 2019
Nurses talked. We listened. Introducing Capella University’s RN-to-BSN FlexPath learning format
October 01, 2015
7 ways Sigma Theta Tau International Honor Society membership benefits nursing students
August 12, 2024
Passing the torch: how nurse leaders can support the next generation
October 25, 2019
Flexibility for a busy lifestyle: an RN to MSN journey with FlexPath
September 15, 2019
OADN executive shares the value of continued education in nursing
November 02, 2018
Advisory board puts Capella at forefront of nursing and health care education
February 15, 2017
Capella students and graduates share their advice for future students | Competency-based education
November 23, 2015
I didn’t go back…I found my way forward: Tarishia’s FlexPath story
October 09, 2015
Ten questions with Capella nursing faculty member Linda Matheson, PhD
April 03, 2015
The PhD sisters: encouragement for women earning doctoral degrees
February 28, 2017
How counseling is changing to meet the needs of today’s older adults
November 18, 2019
Help youth succeed in school and life with a behavioral health degree
August 02, 2019
Collaborative efforts in counseling, clinical psychology, and social work
June 28, 2019
Collaborative efforts in counseling, clinical psychology, and social work
August 21, 2018
The future of education is gaming, says educational psychology faculty member
April 19, 2016
Ten questions with Capella counseling faculty member Leslie Korn, PhD
December 11, 2014
Marriage and family therapy & social work degrees: How to tell the difference
October 03, 2023
The difference between a PhD in social work and Doctor of Social Work
January 11, 2017
Graduate experiences the benefits of a Doctor of Social Work degree
January 12, 2016
Transforming lives: making a career as a marriage and family therapist
March 29, 2019
What you need to know about the Merit-based Incentive Payment System (MIPS)
November 15, 2018
Capella PhD student shares 4 tips on enhancing your social media presence
March 01, 2017
The future of education is gaming, says educational psychology faculty member
April 19, 2016
Four can’t miss EdTech conferences (and one unconference) for K-12 educators
July 15, 2015